参考书籍
1. 雷伟.《脊柱内固定系统应用指南 第2版》第四军医大学出版社.2013年
胸椎椎弓根螺钉技术
一、胸椎的相关解剖







(一)
(二)
(三)
(四)
二、胸椎椎弓根的相关数据







参考书籍
1. 雷伟.《脊柱内固定系统应用指南 第2版》第四军医大学出版社.2013年
参考书籍
1. 史建刚、袁文.《脊柱外科手术解剖图解》上海科学技术出版社.2015年
胸椎椎弓根内固定系统具有良好的三柱固定效果及生物力学性能,在恢复脊柱稳定性上具有明显优势,可适用于造成脊柱不稳的疾病如创伤、肿瘤和畸形矫形等。近年来在脊柱矫形及稳定性重建方面取得了满意的临床效果。
椎弓根内置入
椎弓根外置入(较为简单安全)

患者采用俯卧位。注意于关节处加以敷垫,防止挤压伤。
垫高胸部和髂嵴,使胸部和腹部离开床面,防止静脉回流受阻及呼吸受限并减少术中出血。

切口的选择以手术节段为中心,切口长度应包括上下相邻的正常椎体。
非脊柱侧弯的患者行正中切口即可(图3-4-3)。 
切开真皮层,在后正中线上及两侧可能遇到较为发达的静脉。如无法避免,做好止血(图3-4-4)。切勿切偏,以免伤及脊神经后支。
对于脊柱侧弯患者,首先明确C7棘突和臀裂的垂线,然后在需要手术的节段做直切口。

皮下组织和筋膜之间潜行游离,辨明棘突尖端,找到棘突并分离棘突两侧筋膜。然后在棘突两侧做骨膜下剥离,利于术后该肌肉功能恢复。
如果是儿童患者,可将其软骨性的棘突连同棘间韧带从中间劈开,后用骨膜剥离器将软骨和骨膜一同剥离椎板。

说明:
1. 翻译自Weatherley CR, Emran IM, Newell RL.A modification of the standard midline posterior approach to the intertransverse area of the lumbar spine.Ann R Coll Surg Engl,2010,92(1):19-22.
通过腰椎后正中入路进行后外侧融合需要分离小关节外侧的深部肌肉附着。
目前通过该入路到达lateral gutter的描述并不精确,结果导致不必要的组织损伤和出血。控制出血很重要,对幼儿来说至关重要。

我们提出了一种减少组织损伤和出血的技术,并且已经通过尸体解剖来明确。在过去十多年,一直是我们的标准做法。
在棘上韧带的外侧切开胸腰筋膜(thoracolumbar fascia),用Cobb elevator和a gauze swab将椎旁肌从棘突、椎板和关节突关节上向外侧剥离。
为了暴露横突以进行后外侧融合,继续沿着上关节突的外侧进行解剖直至横突。
我们一直沿骨膜下剥离到关节突关节,该过程几乎不出血,但关节突关节外侧的解剖不太精确,并且出血较多,其出血来源难以识别
Wiltse and Spencer注意到这个区域采用椎旁入路的止血方法存在类似的困难。他们没有在深层显露中明确精确的肌肉解剖结构。
我们注意到小关节外侧的肌肉附着不是弥漫的或随机的,但在显露时,主要分为两束穿过rostrolateral和caudolateral方向,并且其肌腱在小关节囊的外侧直接附着在骨上。

将Cobb dissector放置于这两束肌肉之间并从向外显露横突的步骤中撤回
(Fig. 1)。 

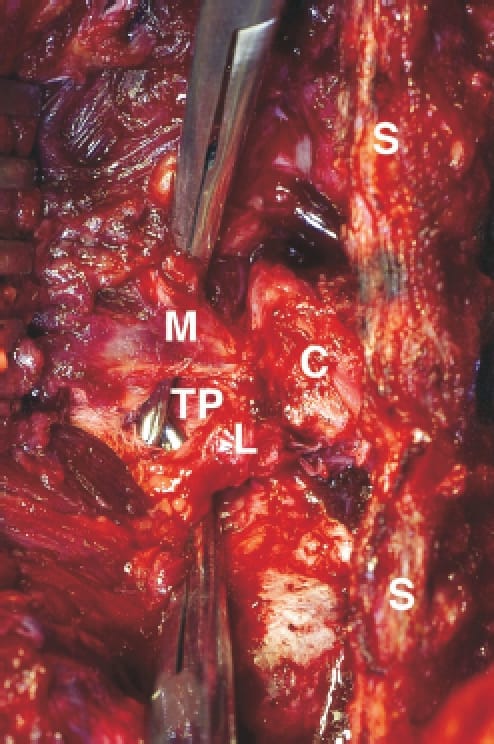
Fig. 1:左侧L4/5水平的手术照片。
- 将弯钳分别在两个肌肉束(多裂肌M和最长肌L)下方通过,上述肌肉束均在小关节囊(C)的外侧附着到骨上。
- L5的横突(TP)位于两个肌肉束之间。
- 中线结构(S)包括棘突、棘间韧带和棘上韧带。
当我们将这两个靠近骨的肌腱附着点切开时,没有出血,我们能够容易地显露下面的动脉。
在标准的后正中入路中,rostral附着点下方的血管是出血的主要来源。
通过我们的显露方法,可以使用长的、带角度的镊子精确地烧灼上关节突的外侧和rostral侧以及横突基底背侧(dorsum)的这些血管。
使用A Cobb dissector on a gauze swab将横突的其余部分暴露到其尖端,尽可能减少出血。
在防腐尸体中,我们确定了在手术过程中暴露的两个肌肉束,它们在小关节囊的外侧附着到骨上,分别是多裂肌和最长肌的一部分。
多裂肌和最长肌占据了腰椎棘突和横突之间的沟槽(gutter)(Fig.
2)。两条肌肉未受干扰的纤维从中线向尾端方向走行。 
多裂肌由一系列重复的肌束组成,从腰椎的棘突和椎板辐射至尾侧两个节段的椎体的乳突(上关节突的下外侧部分)。
最长肌在多裂肌的外侧并且附着点更深。
它由五个肌束组成,每个束都来自副突(靠近乳突,但更偏下外侧,更深)。
上四个肌束形成腰椎肌间腱膜(lumbar intermuscular aponeurosis)并附着于髂骨的后内侧部分。

因此,多裂肌和最长肌都具有靠近小关节囊的bony attachments(Fig. 3):
多裂肌附着于乳突
最长肌附着于副突

最长肌位于更深的平面,其分支的方向不会因手术入路而改变。
然而,多裂肌束的天然方向(natural orientation)发生了变化:沿骨膜下剥离,将多裂肌的肌肉附着点从棘突和椎板上剥离,改变了多裂肌束的方向,从caudolateral变成了caudomedial (Fig. 1,4)。
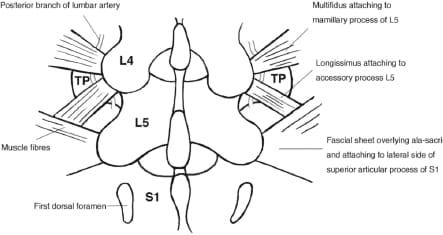
Fig. 4:L4/5和L5/S1水平的肌肉附着图
L4/5处的肌束在L5/S1水平被fascial sheet或腱膜替换,上述fascial sheet或腱膜向外侧延伸覆盖骶骨(sacral ala),被通过脂肪垫与骶骨分开。
多裂肌和最长肌的附着点在腰椎的每个节段都保持相同,但我们注意到在腰骶交界处有所不同。肌束被fascial sheet替代,从S1的上关节突的外侧向外延伸(Fig. 4)。
fascial sheet靠近骶骨附着点的分支从脂肪垫释放脂肪,总是将fascial sheet与骶骨分开。这种解剖结构一直比较恒定,除非L5骶化,此时fascial sheet附着到骶骨化的L5椎体上关节突的外侧面。
Watkins建议用电刀切开小关节囊,显露至横突基底部。
advises extension of the electrocautery cutting of the facet joint capsule down to the base of the transverse process
Weinstein建议继续沿着上关节面(superior
facet)的外侧进行解剖直至横突。 
上述两种描述都能够指导外科医生进入横突平面,但是通过更好地理解该入路的深层解剖结构,将有助于减少出血和组织损伤。
我们发现,有两个主要且不同的骨骼肌肉附着点:乳突和副突。这种模式在整个腰椎直到L5/S1交界处都是保持一致的。
此外还发现,上述模式在L5/S1水平被筋膜层或腱膜所替代(从关节囊延伸至上关节突外侧面),这种替代也往往是稳定的。我们没有发现既往有文献对该筋膜进行描述。
筋膜位于相同的深度并且具有相似的到骨骼内侧的附着点,这表明该筋膜层可以代表多裂肌和最长肌最下面肌束的融合。这个节段的解剖学差异可能是腰骶部水平相对缺乏运动的标志。
或者,基于显露的筋膜所在的部分平面,它可以代表髂腰韧带复合体(iliolumbar ligament complex)的浅表结构。
说明:
1. 翻译自Frederic W. Platt MD,Geoffrey H.Gordon MD FACP FAAPP.Field Guide to the Difficult Patient Interview.LWW,2004.
有效的交流应建立于对患者个性范畴充分理解的基础上,而绝不单单是患者躯体上的临床问题。
因此,会谈开始时你头脑中的第一个问题应该是:他(她)是一个什么样的人?
当医生们被问及是怎样开始与患者对话时,通常可告诉我们三种情况:
在会谈的开始阶段,用一点儿时间询问一些患者的社会史情况,可能会密切你与患者之间的关系。
患者中的绝大多数是很愿意用简洁的几句话让你了解他们所认为较为重要的事情,但也有极少数的病人很可能并不清楚他该说什么,这时你可以用一些简短的话题来帮助他们:
医生:看病之前,我想知道一些您的个人情况。
患者:你的意思是什么,大夫?
医生:恩。比如您住在哪里?谁是您生活中的重要人物?您做何种工作?闲暇时喜欢做些什么?您知道么,这些对了解您都是很重要的。
在随后的医疗接触中,你可以继续在个人层面上与患者进行沟通表明除了关注患者的器官和疾病之外,你对患者整体健康及其整个生活都感兴趣。
医生:Hi, Joe, how are you doing?
患者:Fine, doctor. Pretty good.
医生:I remember that last time you were here you said that you were planning a trip to Chicago. How did it go?
患者:Great, Doc. We had a lovely visit. Saw all the relatives and took in a Cubs game at Wrigley Field. Thanks for asking. I’m amazed you remembered.
注:你真的记得这一切吗?不,当然不。但你确实看了一眼last chart note,上面记录着“患者计划去芝加哥旅行”,帮助你在今天记忆起来。
在开始交谈之前,要设法获取与患者关注和期望有关的全面情况(complete list of the patient’s concerns and desires)。
只有极少数的病人是仅为一个问题来看医生的。他们可能是因为某一个问题的驱使来与你见面,但这个问题可能伴随着各种各样的补充问题。对于每个问题,大多数患者都有症状,要求和问题,可以提前对这些问题做好准备。
当你获知患者的基本个人需求后就可开始你的检査了:
只有当他(她)在你询问“还有什么?”后,至少两次再回答你“没有了“时,你才应确认已获知了对方的全部意图。
只有当你了解了他的一些难以抓住要点的问题,随后你才能准备开始惯例的会谈,如询问哪一个是所有问题中最苦恼的,或去追索他(她)的主诉。
然后,你可能需要与患者商讨一个双方共识的议程,尤其是当你与病人之间在所谈问题的重点上存有分歧时更应如此。
医生:好吧,A先生,我明白您有6个问题,但我最关心的是第3个问题。即胸痛。我听您讲这是您尤其感到不舒服的问题,但您又说还有皮疹、腹泻及膝盖发酸的症状。我们不大可能把这些问题都解决。因此,我想今天我们着重解决胸痛的问题。您是不是觉得胸痛是最重要的?
帮助病人表达他所关心的问题可有助于使你免于陷入“顺便问一下,医生”综合征的干扰。尤其在你想要结束询问并几乎就要离开之前,这种综合征可能阻碍病人表述他最主要的问题或症状。
例如此时病人才说“顺便问一下,大夫,对呕血的病人您将怎么处理?”
“顺便问一下”表明你可能在一开始就没有完整引出患者的议程(complete agenda),因此也无法确定你是否明确了主诉。

如果你能提供诊治的规划和要点,患者将会很愿意按照你说的去做。
很多病人都是第一次来到诊所看病,他们很可能从未有过接受全面体格检査的经验。因此,他们可能不明白作为一个医生将对他们的健康所应具有的重要责任,或者也不清楚医生在尝试有效治疗前必须要做出诊断,因此你必须向他们介绍这些情况。
医生:Mrs. S., I want you to take the first few minutes to tell me what you think is most important about this. Then I’ll want to ask you some questions before I examine you.
过一会儿
医生:好的,S先生。我想我清楚您今天为什么来这里了。下面我要做的是一项仔细的体检,随后我们再讨论时什么原因造成您的不适以及我们将可以做些什么。对这一点您有什么问题吗?
患者:体检?你能否只给开点镇痛和止咳药?
医生:我想那很简单。但是我还需要更多的资料来确定诊断。然后才能做出合理的治疗方案。这就是为什么必须进行体检的原因。
患者:奥,我猜想那样病情才能清楚了。不然的话,你就会像拜尔医生那样通过电话就给我开药了。
你的办公职员或健康计划应能够帮助你的病人在开始看病之前就已经了解如何做好就诊的准备。
在患者进行陈述时,成功的医生总是能够表示他对患者病史的兴致,并且能够认真地倾听。
Mischler教授在对医患交流的系统分析结果中指出:在对话中医生和病人好像是在讲两种不同的语言(Mischler EG.医学讲座,1984)。
我们的工作包括将患者的语言翻译成一组有助于诊断推理和临床判断的客观信息。
此外,听取患者的开场陈述,我们可以得出他所能够向我们呈现的信息类型的结论:症状,想法,感受和价值。
医生和患者话语的这种平衡一直存在。
在谈话中,我们从开放式询问(open-ended inquiry)开始,然后逐步缩小我们的关注点和质疑。
我们在会谈的各个部分之间使用:
但是,患者的故事在会谈的一开始就可能会给我们带来麻烦:
医生:请讲一下您胸痛的情况
患者:好点,但我得先让你知道去年我们从伦敦回来时发生的事情。
医生:伦敦?
患者:是的。航班出了点问题。我们是绕道旧金山飞回来的。这看起来并没有什么不好。只是多飞了一些航程,但在旧金山又因下雨耽搁了3个小时。我们因此不得不步行去了机场旅馆。你知道那里的立体交叉公路有多难绕行么?
医生:我知道了。您认为是在旅行中发生的事件引发了您的疼痛。但您能否先讲一讲您目前所感到的与胸痛有关的症状?比如疼痛的部位,什么时候发作?哪些原因可能会使疼痛加重或好一些?
然而,尽管我们想要了解的更多,伹却很少有机会能得到恰到好处的症状依据。
最后要提到的是,医生与患者共同参加完成病史的组织工作可以使你们实现更好的共识,但如果我们未能在与患者的初次会谈中做好倾听,就将不会达到这样的效果了。
像这样组织一个完整病史的过程,其实就是在患者叙述病情和医生确认病因之间来回斟酌的过程。
你可以通过向病人询问更为准确的解释来增进你对他供述的了解,也可以通过向病人再次重复他所对你讲的内容来表示你在倾听及努力理解他。
Sullivan把这种复述比做如同跟随一个人穿行在黑暗的通道中不断地询问“你在哪里?” 一样,以此作为调整方向的反应。
通过对患者身上所反映出的生物医学及社会心理问题的深思(reflection),将能提高我们判断的准确性,从而引导更为合理的疾病诊断。
对患者认识观、价值观及感受方面的反思是移情交流(empathic communication)的基本方法并直接有益于对患者的治疗。
请认真理解下述应用深思(reflection)或“简要概括(short summaries)”的范例:
#### (1)组织议程
患者:就是这些,医生。我胸痛,膝盖也痛,而且看来咳嗽也可能不会好了。
医生:好的。如果我没有听错。您感到胸痛、膝盖痛和咳嗽,还有其他不适么?
患者:是的,还有一件事。最近我的性生活方面也差了很多。其余没有了。
医生:我知道了,您胸痛、膝盖痛、咳嗽及性生活也有问题。还有吗?
患者:就这些,医生。这还不够么?
医生:听起来好像是差不多了。
#### (2)识别症状
患者:我疼了一个星期了。而且今天早晨醒来时又出现莫名其妙的皮疹,我难受极了,皮疹刚好就在右侧疼痛的地方。
医生:那么听起来是您腰部的右侧已经痛了一周,然后今天又突然出现了皮疹。
患者:是这样的。
#### (3)确认认识观
患者:我觉得我是得了痛风病,我认为我需要服用一些秋水仙碱或其他药物。
医生:那么您在告诉我的是您认为得了痛风,而秋水仙碱能治疗您的病。
患者:正是如此。
#### (4)确认价值观
患者:其实我真的不想偷懒。这件工作我刚刚干了一个月。我并不想让别人认为我是想逃避工作。
医生:我当然明白,您不想偷懒。这一点对您很重要。
患者:你说的一点不错。
#### (5)确认患者的感受
患者:医生,不知怎么的了。自从我的爱犬死后。一个月以来,我一直很悲伤。我知道那条狗确实是老了,事情已经只能如此。可在此之前每当我回家时它总是在那向我打招呼。但现在我和妻子回家时,却再也没有谁会问候我们了,我已经真的失去了我的狗。
医生:我能理解,您失去了爱犬。而您为它的死而感到悲伤。
患者:是的,确实如此。
我们的经验是,体现深思的倾听或移情(Practicing reflective listening)并不会过多地延长会谈的时间,而事实上却可能节省我们的时间。如果患者不能确信已被倾听及理解,那么他(她)则会再次重复所讲的内容。
医生:So feeling pretty sad and forlorn(孤立无助的), eh?
患者:No, not so sad as really angry. They shouldn’t have abandoned me that way.
在这种情况下,医生可以纠正他的误解:
医生:I see. Not so much sad as angry. I can imagine how you’d feel that way.
要善于表现你的关心但又不要过分的表达。你也不必对患者的每个症状、想法或感受都表示共鸣,但你应为了表示移情而不时地做出一些反响。总而言之,你千万不要错过这个最重要的表现机会。

一直觉得科研是自己的薄弱环节,发表在国外的文章也是清一色的临床内容。可能有以下原因:
对科研的重视程度远不及临床;
选择恰当的切入点比较困难;
基础医学的发展令人目不暇接, 常有跟不上的感觉;
条件、经费有限。
当然第4点与前面的1、2、3点是互为因果的
一直认为临床研究也是研究,临床科研也是科研。所以一直希望这方面的工作能够解决临床问题,目前正在开展以及计划开展的研究涉及几方面的内容,基本是临床基础研究。将来如果条件及经费具备,可能会开展更基础一些的基础研究。
脊柱生物力学的研究开始较早,也有了一定基础,如条件具备也可能会对生物力学的某些基本问题作些工作。
骨质疏松与骨折关系的临床流行病学研究、骨质疏松与腰背痛关系的研究、骨关节炎与骨质疏松关系的研究、脊髓损伤与骨代谢异常、脊柱的应力分布与骨密度的关系、MRI对于骨质疏松性椎体骨折的诊断价值等等,还因此获得了中国骨质疏松基金会颁发的学科成就奖(对此我非常珍视,因为这是内行评出的奖)。但创新不够,还要加把劲。## 三、读万卷书,行万里路 1. 读万卷书,行万里路。意思是要多读书,多实践。这是我自己的深切体会,在这里提出来与大家共勉。 2. 我以为,定义一个好的临床医生可有3个境界。 * 首先,应该掌握本专业基础知识、基本理论和基本技术; * 再进一步,要在学术上不断提高,跟上国内国外学术发展的步伐; * 更高的要求则是形成自己的特色并被同行所承认,在前人成就的基础上有所发现有所创造。 3. 这3个境界中第3个是最难的,但却又是以前两个境界为基础的。不熟练掌握本专业的基础知识、基本理论和基本技术,再进一步发展其实是非常困难的。 4. 近年来与国外的交流逐渐增多,感觉我们与国外的同行存在着很大的差距,这一差距在起跑线上就已经存在了。国外在医学院学生的招生、培养,住院医生以及专科医生的培养早已经形成了一整套行之有效的制度,而我们国内在这方面就远不如人家。 5. 怎么办?多实践的重要性人人都懂,但对于读书学习的重要性和必要性好象就不那么清楚了。 * 例如,作为脊柱外科医生,你对于脊柱外科的常用分类方法、常用评分标准是不是很熟悉呢? * 对于各种手术的适应证是不是已经了如指掌了呢? * 再比如,为什么直到现在还有医生搞不清楚爆裂性骨折和压缩性骨折的区别呢! 6. 随着学科的发展,有关基础知识、基本理论和基本技术的范围也在扩大,例如脊柱的MRI检查。 * 我在丁香园上看到不少医生由于缺乏脊柱影像学诊断的基本知识,往往是凭感觉就觉得象是某个病,而却又讲不出太多的依据。为什么不去翻翻书熟悉一下这些疾病的MRI表现呢? * 如果某些疾病根据影像学表现就可以排除的话,就没有必要去作试验性治疗、也没有必要去作探查性手术了。 7. 了解学术动态的重要性。对于脊柱外科的主要期刊(例如Spine)你是不是每期都要浏览一下呢? * 你也许会说我只是个小医生。但老医生都是从小医生成长起来的。 * 读书的习惯也是从小医生时就应该养成的,否则将来凭什么去带小医生呢? 8. 读万卷书和行万里路并不矛盾,医生所遇到的第一个病例常常是在人家的论文中,借鉴别人的经验,丰富自己的阅历,何乐而不为呢? 9. 读书读多了,就有一个怎样消化的问题。现在大家的外语水平越来越高,但绝不应将自己限制在 “国际倒爷”的层次上。尤其是大医院的医生,大学附属医院的医生,都应该向最高的境界努力。在国外的大学里,这第3个境界就是评教授的标准。## 四、论文 ### (一)SCI论文 1. Dai LY, Xu YK, Zhang WM, Zhou ZH, Wang YJ. Effect of posterior structure resection on lumbar spine stability: a preliminary biomechanical study. Chin Med J 1988; 101(4):272-276.2. Dai LY, Xu YK, Zhang WM, Zhou ZH. The effect of flexion-extension motion of the lumbar spine on the capacity of spinal canal: an experimental study. Spine 1989; 14(5):523-525.3. Dai LY, Xu YK, Zhang WM, Zhou ZH. Influence of flexion-extension motion of lumbar spine on lumbosacral dural sac: an experimental study. Chin Med J 1991; 104(6):498-502.4. Dai LY, Tu KY, Xu YK, Zhang WM, Cheng PL. Effect of discectomy on the stress distribution in lumbar spine. Chin Med J 1992; 105(11):944-948.5. Dai LY, Jia LS. Radiographic measurement of the prevertebral soft tissue of the cervical vertebrae. Chin Med J 1994; 107(6):471-473.6. Dai LY, Jia LS, Xu YK, Zhang WM. Cruciate paralysis caused by injury of the upper cervical spine. J Spinal Disord 1995; 8(2):170-172.7. Dai L, Ni B, Jia L, Liu H. Lumbar disc herniation in the patients with developmental spinal stenosis. Eur Spine J 1996; 5(5):308-311.8. Dai LY, Jia LS. Multiple noncontiguous injuries of spine. Injury 1996; 27(8):573-575.9. Dai L, Jia L. Acute central cervical cord injury presenting as only upper extremity involvement. Int Orthop 1997; 21(6):380-382.10. Dai L. The relationship between vertebral body deformity and disc degeneration in lumbar spine of the senile. Eur Spine J 1998; 7(1):40-44.11. Dai LY, The relationship between osteoarthritis and osteoporosis in the spine. Clin Rheumatol 1998; 16(1):44-46.12. Dai LY, Jia LS, Ni B, Yuan W, Liu HK, Hou TS, Zhao DL, Xu YK. Diagnosis and treatment of acute central cervical cord syndrome. Chin Med J 1998; 111(4):351-353.13. Dai LY. Disc degeneration and cervical instability: correlation of magnetic resonance imaging with radiography. Spine 1998; 23(16):1734-1738.14. Dai LY, Ni B, Yuan W, Jia LS. Radiculopathy after laminectomy in cervical compression myelopathy. J Bone Joint Surg [Br] 1998; 80(5):846-849.15. Dai LY, Yuan W, Ni B, Jia LS, Zhao DL, Xu YK. Traumatic disruption of the transverse atlantal ligament. NeuroOrthopedics 2000; 27(1-2):37-41.16. Dai LY, Jia LS. Central cord injury complicating acute cervical disc herniation in trauma. Spine 2000; 25(3):331-336. 17. Dai LY, Yuan W, Ni B, Jia LS. Os odontoideum: etiology, diagnosis, and management. Surg Neurol 2000; 53(2):106-109.18. Dai LY, Yuan W, Ni B, Liu HK, Jia LS, Zhao DL, Xu YK. Surgical treatment of nonunited fractures of the odontoid process: with special reference to occipito-cervical fusion for unreducible atlantoaxial subluxation or instability. Eur Spine J 2000; 9(2):118-122.19. Dai LY. Disc degeneration in patients with lumbar spondylolysis. J Spinal Dis-ord 2000; 13(6):478-486.20. Dai LY. Remodeling of the spinal canal after thoracolumbar burst fractures. Clin Orthop 2001; 382:119-123.21. Dai LY. Acute central cervical cord injury: the effect of age upon the prognosis. Injury 2001; 32(3):195-199.22. Dai LY, Jia LS, Yuan W, Ni B, Zhu HB. Direct repair of defect in lumbar spondylolysis and mild isthmic spondylolisthesis by bone grafting: with or without facet joint fusion. Eur Spine J 2001; 10(1):78-83.23. Dai LY. Orientation and tropism of lumbar facet joints in degenerative spondylolisthesis. Int Orthop 2001; 25(1):40-42.24. Dai LY. Mechanism associated with thoracolumbar burst fractures: a biomechanical study. Chin Med J 2002; 115(3):336-338.25. Dai LY. Low lumbar spinal fractures: management options. Injury 2002; 33 (7):579–582.26. Dai LY, Yao WF, Cui YM, Zhou Q. Thoracolumbar fractures in multiply injured patients: diagnosis and treatment--A review of 147 cases. J Trauma 2004; 56(2):348-355.27. Dai LY. Significance of prevertebral soft tissue measurement in cervical spine injuries. Eur J Radiol 2004; 51(1):73-76.28. Dai LY, Ye H, Qian QR. The natural history of cervical disc calcification in children. J Bone Joint Surg [Am] 2004; 86(7):1467-1472.29. Dai LY, Jin WJ. Interobserver and intraobserver reliability of the Load Sharing Classification in the assessment of thoracolumbar burst fractures. Spine 2005; in press30. Dai LY, Jiang LS, Wang W, Cui YM. Single-stage anterior autogenous bone grafting and instrumentation in the surgical management of spinal tuberculosis. Spine 2005; in press31. Dai LY, Zhou Q, Yao WF, Shen L. Recurrent lumbar disc herniation after discectomy: outcome of repeat discectomy. Surg Neurol 2005; in press
出席国际会议的想法实际上由来已久。改革开放使走进新时代的中国以前所未有的速度开始了现代化的进程,在逐渐与国际接轨的同时,中国的科技工作者也开始了与我们以往并不了解或者了解甚少的国际社会的交往。
层出不穷的新理论、新技术被越来越多越来越快地介绍进来,而我们也确确实实地感受到了我国医学科学事业的发展和变化。在这种形势下自然而然地会提出这样的问题:我们和世界先进水平究竟相差多少?我们已经取得的大大小小的成就,在和国外同行的竞争和竞赛中到底处于什么地位?
出席国际会议无疑是了解最新信息以及与国外同行交流的极好机会。记得是十几年前,我将论文投寄给日本脊柱外科年会并被接受为大会发言,但当时的审批制度使得与会根本不可能成行。此后,在相当长的一段时间内,我虽然陆续在国外期刊上发表了一些论文,但也没有再向国际学术会议投稿。其间参加过两次在国内举办的国际学术会议并在会议上发言,这两次会议的国外代表仅占较小比例,但他们的到来仍然给会议注入了清新的空气,使我领略到外面世界的精彩。
新世纪开始之际,我告别了生活、工作已20余载的军营。到新的岗位报到后,我在填写职称晋升表格的同时即向AAOS寄出了我的论文。几个月后收到了AAOS主席的邀请信以及论文被年会接受作为墙报张贴的通知。这篇论文虽然没有被接受为大会发言,但毕竟是我被AAOS所接受的第一篇论文。
如果说在接到邀请信时我的心头曾涌起了一丝喜悦和一点满足感的话,几个月后的美国之行却使我不得不面对严酷的现实。在旧金山AAOS第68届年会展厅的墙报中交流的国际论文,只有孤零零的一面五星红旗。这时我才如此深切地感受到我们与国外同行的差距和我们在国际上所处的地位。
从美国归来后,我又向AAOS的下一届年会寄出了我的新的论文,再次收到AAOS主席的邀请信和论文被接受为墙报的通知,2001年尽管我所发表的SCI论文数并不多,但仍然名列全国医药界第1名。
2002年初,我又向CSRS和AAOS投去了我的论文。在投稿之前了解到,CSRS(颈椎研究学会)是目前国际颈椎研究方面最具权威性的学术组织,也是著名的Spine杂志的主办单位之一。申请CSRS的会员要求比较严格,其条件之一就是必须参加一次CSRS年会并有论文被会议接受。随后CSRS和AAOS均接受了我的论文在会议上报告,于是我就有了在CSRS和AAOS第一次发言的经历。也许这个第一次是那么微不足道,但对于我却是意义深远。我确信自己所走过的路是正确的,所付出的努力并没有白费。在CSRS的展厅里,见到了刚刚出版的第10版Campbell骨科手术学,我在10多年前发表的一篇论文又被这部名著所引用(第8、9版都曾引用过这篇论文)。
几次赴美参加学术会议的经历,使我深切地认识到我们与国际先进水平的明显差距。诚然,我们也在进步,我们前进的步伐比以往任何时期都要快,但工作太缺乏原创性,常常只是停留在模仿和跟踪上。尽管有一些国内的同行一直在努力工作并取得了可喜的成绩,但这些成绩却不为国外同行所知,也缺乏国际公认的标准和规范的检验。在国际学术论坛上的声音还很微弱,在权威期刊上发表的论文还太少太少。因此,我们的任务还相当艰巨,路途还非常漫长。唯有更加勤奋和努力,才有可能在国际学术讲坛上占有一席之地。
本文不仅仅是对以往工作的回顾,而且标志着新的努力的开始。
###(一)脊柱侧弯方面的进展 1. 我们新华医院早在20世纪70年代就开始了脊柱侧凸的手术治疗,而我本人在国外进修期间也是以脊柱畸形为主要内容。当时导师给我布置的工作是总结先天性脊柱侧凸的临床资料,花了几个月的时间,片子也读了几千张。所以现在虽然主要方向不在脊柱畸形上,但对这一问题一直有兴趣,并手术治疗了一些病例。 2. 这里主要讨论特发性脊柱侧凸。特发性脊柱侧凸的治疗选择常常涉及到很多因素。手术还是不手术?如果手术,主要的目的是什么?是矫正畸形,还是其他:防止畸形进一步加重?重建躯干平衡?或是为了以后的腰背痛问题、呼吸困难问题?或者只是为了美观。对于这些问题在决定手术前都应该有一个比较全面的考虑。这就需要医生对疾病的自然史有一个清晰的认识,就是说要知道对于这样一个具体的病例如果我不开刀会产生什么样的后果。这方面的研究往往需要花费大量的精力,因而也更有价值。比较引人注目的是著名脊柱外科专家Stuart Weinstein等去年发表在JAMA上的一篇文章。 > Weinstein SL, Dolan LA, Spratt KF, et al.: Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study. JAMA 2003; 289:559–567. 他们报道了117例未治疗的特发性脊柱侧凸50年随访结果,并与62例志愿者作对照。患者最后随访时年龄为54-80岁,平均66岁。研究结果提示,晚发的特发性脊柱侧凸(late-onset idiopathic scoliosis)患者虽未经治疗, 其远期随访结果仅在腰背痛和外观方面与对照组有一定差距,其他健康及功能参数均与对照组无异。如此长时间的随访资料,得来实属不易。 3. 特发性脊柱侧凸手术治疗的关键是融合范围的选择。过去主要依据在Harrington系统基础上提出的King分类,选择性融合后出现了一些失代偿的病例。现在Lenke等又提出了新的分类:
> Lenke LG, Betz RR, Harms J, et al.: Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg [Am] 2001, 83:1169–1181. 所考虑的问题更加全面,对选择融合范围的指导性更强,近几年围绕Lenke分类有几篇文章, 当然也提出了一些意见。问题是如果分类覆盖的范围越大就会越复杂,也越难掌握。4. 此外,前路胸腔镜手术、前路开放手术以及椎弓根螺钉的应用等,究竟会给手术治疗带来什么影响都是值得关注的问题。总的原则是要在融合范围尽可能小的前提下取得满意的效果。在我们这个国家还有一个比较突出的问题,那就是怎样更省钱?###(二)请问往SPINE杂志或类似的外国期刊投稿时有何技巧?(不考虑文章内容,实验方法等客观的因素,只考虑投稿的技巧,即若何能让编辑考虑发表)1. 技巧始终是第二位,有新意永远是第一位的。
* 首先要告诉审稿人你的内容是有新意的(但不能胡吹)
* 其次要让人知道你的工作既是有新意的又是重要的
* 根据创新性和重要性的不同你所能发表文章的档次也有所不同2. 要把与你文章关系密切的文章尽可能都读过,在前言部分综述一下,告诉人家现状、不足,和你的假设和本文的目的(要具体有针对性)。3. 材料和方法:要详细。4. 讨论:
* 要强调你的发现是什么?
* 有什么意义?
* 与别人的工作有什么不同?
* 本研究的不足和缺陷是什么?5. 参考文献:重要的都要列出,列出的都要读过全文。6. 别在小处让人家扣分,比如不要写错别字。###(三)怎么读书1. 要读好书,读公认的好书。我曾花了1年的时间读完了坎贝尔手术学,这是骨科医生的入门书。如果是脊柱外科医生还要读脊柱外科的专著。 2. 接下来就是读期刊,对于脊柱外科的重要文章要熟悉,对重要的期刊(如Spine)应养成定期阅读的习惯。 3. 对于书和论文后罗列的重要参考文献也应找来阅读。对于重要的作者甚至要作追踪。 4. 读书的习惯要早早养成,不能以忙为借口拒绝读书。曾问过一个有名的脊柱外科医生(已经近60岁)你每天下班这么晚读书是在什么时候?他的回答是: “In the morning.” 5. 读万卷书只是比喻,读过了还要从书堆里跳出来。对读过的东西要消化,要有自己的想法,新的想法。
###(四)多节段脊柱全椎板切除术对脊柱稳定性的影响?植骨融合内固定的指征是什么?1. 这是我硕士研究的课题。椎板切除对腰椎的稳定性是有影响的,但是不是都到了需要融合的地步。我觉得需要具体病例具体分析。有许多因素影响术式的选择。 * 是否同时切除关节突关节:切除关节突关节稳定性会更差,全部切除比部分切除差。一般不是全切除不稳的发生率不高。 * 年龄和职业。老年患者一般不需融合。 * 体重。 2. 我的观点: * 尽量避免全椎板切除 * 尽量避免切除关节突关节 * 如果不可避免,中青年患者,体重大的患者,还是需要融合。
###(五)
###(六)
###(七)
###(八)
###(九)
说明:
1. 参考自Yue BY,le Roux CM,Corlett R et al.The arterial supply of the cervical and thoracic spinal muscles and overlying skin: Anatomical study with implications for surgical wound complications.Clin Anat,2013,26(5):584-91.
有大量的文献关于供应脊柱肌肉和皮肤(spinal muscles and overlying skin)的脉管系统。
髂肋肌(Iliocostalis)



最长肌(Longissimus)



棘肌(Spinalis)



Splenius capitis muscle
Splenius cervicis muscle


semispinalis capitis
semispinalis cervicis
semispinalis thoracis
![]()






头后大直肌(Rectus Capitis Posterior Major)
头后小直肌(Rectus Capitis Posterior Minor)


头上斜肌(Obliquus Capitis Superiorta)
头下斜肌(Obliquus Capitis Inferior) 

棘间肌(Interspinales)
回旋肌(Rotatores)
多裂肌(Multifidus)



transversospinales是人体背部的一组功能肌群。它们的联合作用是脊柱的旋转和伸展(extension)。包括:
将套管(Cannulae)插入每一个肋间动脉并用缝线固定。
导管(Catheters)充气并固定在颈总动脉和锁骨下动脉内。 

将样品浸入40℃的温水中,水浴1小时从而使血管扩张最大化。
将过氧化氢注入每一个肋间后动脉(posterior intercostal a.),锁骨下动脉(subclavian a.)和颈总动脉(common carotid a.)。
然后将样品再次浸入温水中,水浴1小时。根据先前描述的技术制备四氧化三铅/奶粉混合物 (Pan et al,2010)。
(36克精细研磨的奶粉,200克四氧化三铅[Pb3O4],120毫升水)
以逐步、选择性的方式注入四氧化三铅/牛奶混合物。
以脉冲方式进行注射(模拟自然动脉搏动以最小化降低血管破裂的风险)(Rees和Taylor,1986)。
然后将样品在冷藏室中储存至少5天,以便使四氧化三铅混合物在解剖前稳定在动脉内。
将造影剂混合物注入到所有样本中,在新鲜的和防腐处理后的样本中产生充分灌注的X线照片。
颈深动脉和superficial cervical
arteries始终被观察为颈椎区域椎旁肌和皮肤的主要供应动脉 (Fig. 1)。 


颈深动脉起源于T1肋椎关节前的肋颈干(costocervical
trunks)。颈深动脉在颈椎的后缘上方走行至transversospinales肌肉组和竖脊肌的前部,与枕动脉(occipital
artery)吻合。 
The transverse cervical artery来自甲状颈干,其分支为:
1.Superficial branch
2.Deep branch/dorsal scapular artery/descending scapular artery
Deep branch通常来自锁骨下动脉(第二或第三段),但也有25%来自transverse cervical artery。在这种情况下,Deep branch也被称为the deep branch of the transverse cervical artery。而Superficial branch和Deep branch的结合部被称为cervicodorsal trunk。



Descending branch (also known as superficial cervical artery,供应斜方肌的中间和外侧部分)

- orange: Superior or upper fibers of the trapezius
- red: Middle fibers of the trapezius
- purple: Inferior or lower fibers of the trapezius
在两个标本中,cervicodorsal trunks源自T1水平的锁骨下动脉的甲状颈干。
在所有标本中,椎动脉始终源于T1椎体前外侧的锁骨下动脉。




在该研究中未注射颈外动脉,并且在两个样本中,通过椎动脉与枕动脉之间的吻合支灌注枕动脉。

Cross sectional X-rays of the C1/2 and C7 vertebral levels following selective injection of the subclavian and common carotid arteries.
肋间后动脉(posterior intercostal a.),superior intercostal artery和肩胛背(dorsal scapular a.)是胸椎椎旁肌和皮肤的主要动脉供给(Fig. 3)。
supreme intercostal artery/the highest intercostal artery/superior intercostal artery
通常来自肋颈干,通常发出first and second posterior intercostal arteries,供应相应的肋间隙。



Cross sectional X-rays of the T2 and T10 vertebral levels following injection of the subclavian, common carotid, and posterior intercostal arteries.
在所有标本中,superior intercostal
artery起源于T1水平的肋颈干(costocervical
trunks),并且沿前外侧下降至椎体。其沿着T1,T2和T3处肋骨的肋沟(costal
grooves of ribs)。 
在所有标本中都可以观察到,superior intercostal arteries对斜方肌和皮肤的贡献最小。
superior intercostal arteries在椎板后面有两个较大的吻合通道。
肋间后动脉(posterior intercostal a.)




肩胛背动脉(dorsal scapular arteries)
在颈背部和胸背部中,脊柱肌肉在每个椎体水平按分段的方式由分支供应(segmental fashion at each vertebral level)。
在胸背部,两条小血管始终为dorsal intercostal artery perforators(来自superior intercostal a.和肋间后动脉)提供choke anastomoses。
这两个血管始终位于棘突底部的侧面,位于椎体的椎板后面(Fig. 4)。
供应左侧和右侧椎旁肌的动脉在棘突间韧带内始终相互吻合。
Cadaveric studies have revealed that cutaneous perforators are linked by either reduced-caliber "choke" arteries, or by vessels without change in caliber, the true anastomoses.

- Anteroposterior X-ray image of the thorax following injection of the superior and posterior intercostal arteries (both orange).
- 红色箭头指向两个吻合血管,这两个吻合血管提供dorsal intercostal perforator arteries之间的纵向连接。
先前研究的X线照片是从全身输注造影剂混合物的样本中产生的(Crock,1977; Taylor和Palmer,1987; Houseman等,2000; Minabe和Harii,2007)。
相比之下,本研究采用逐步注射造影剂混合物以及每个椎体水平的标本成像,以允许绘制血管支配区域和血管吻合区域。通过这些对比X线片显示的动脉解剖结构,以及颈背部和胸背部区域之间的比较,能够彻底地研究局部循环障碍可能导致术后伤口并发症的可能机制(Fig. 5)。

Fig. 5:后正中入路的脊柱脉管系统和手术视野的图示。
- 在选择性注射锁骨下动脉和颈总动脉后,C3椎体水平的血管:vertebral (purple), deep cervical (red), and superficial cervical arteries (green)
- 选择性注射肋间后动脉后,T10椎体水平的血管:posterior intercostal arteries
- 箭头所示为预计的手术区域。
说明:
1. 参考自Moghimi MH, Leonard DA, Cho CH et al.Virtually bloodless posterior midline exposure of the lumbar spine using the "para-midline" fatty plane.Eur Spine J,2016,25(3):956-62.
尽管随着微创腰背部手术的普及和进步,但腰椎的标准后正中入路(posterior midline approach)仍然是广泛解决脊柱疾病的最常见和最实用的方法。
腰椎后正中入路由埃伊那岛(Aegina)的Paulus于公元7世纪首次描述,后来于1886年由Mac Ewen首次演示。这种方法在脊柱外科中被教条般接受,几乎没有任何变化。因此,随着时间的推移,后正中入路的方法几乎没有任何修改,甚至对该区域的外科解剖结构的评估也较少。
根据其在无数教科书中的重复描述,它要求对从棘突到椎板的所有肌肉和组织进行细致的骨膜下解剖(subperiosteal dissection),并横向延伸到峡部(pars interarticularis)和小关节(facet joints)。

对于计划后外侧融合(posterolateral fusion)的病例,使用传统方法时,一旦从棘突上剥离椎旁肌,则必须“剥离”椎板外侧剩余的肌肉以暴露横突。虽然进行这种暴露的工具从电刀(electrocautery)到subperiosteal Cobb elevators不等,但是解剖平面保持不变。

一般情况下,为了获得充分的手术视野,需要剧烈撑开已经剥离的肌肉和组织。这种显露方法的出血可能是由于穿孔血管和棘突旁静脉(perforating vessels and paraspinous process veins)的破坏造成的。


已经有文献报道改进的后正中入路。
由于对传统的开放的后正中入路进行显露导致的失血感到沮丧,作者考虑了可以减少出血的技术改进。

基于这一经验,为初次(非翻修)腰椎手术开发了类似的显露技术。

![]()


本文有三个目的。
患者俯卧位,用手术刀沿需要暴露的节段的棘突正上方做纵向的正中切口。
此后,用电凝(electrocautery)做进一步的解剖。
通过皮下脂肪平面暴露deep lumbar fascia。
在每个阶段,都实现了精细止血。
Self-retaining Weitlaner或cerebellar retractors用于撑开皮肤和皮下组织。


不是直接在后正中线切开deep lumbar fascia,而是在棘突的任一侧纵向切开筋膜,留下约5mm的组织袖(cuff of tissue)(Fig. 1)。


在筋膜深处,横切多裂肌的一层薄薄的肌肉附着点,露出了旁正中的脂肪平面(para-midline fatty plane)(Fig. 2)。

使用电凝在这种脂肪组织内继续解剖,紧贴深部椎旁肌的内侧。当平面在前外侧稍弯曲时,进一步解剖显露小关节囊,通过松开周围肌肉而不损坏小关节囊本身(Fig.
3)。 


当所有手术节段的小关节囊都显露之后,可以在其最下方的外侧进行解剖以显露横突。透视定位无误后,就可以置入deep
retractors。 
在第二阶段中,可以在骨膜下显露中线结构,包括椎板,棘突和峡部。
2014年9月至2015年5月,由高年资外科医生进行的1~3节段(即运动节段)初次(即先前未手术)腰椎手术的50名患者进行了前瞻性登记。
对所有患者均使用旁正中脂肪平面方法。不包括:
收集的数据仅为:
使用Neptune 2抽吸装置(Stryker Surgical,Kalamazoo,MI)在术中测量出血量,其需要在开始记录体积之前收集20cc的液体。

50名患者的MRI检查由经验丰富的高年资神经放射学家独立检查,以确定旁正中脂肪平面的存在。
对于多节段的患者,分别评估每个融合节段。
所有患者都有矢状面和横断面的T1和T2加权图像,7例缺乏横断面T1序列。

然而,脂肪平面在横断面T2加权图像上能够很好地获得可视化,在缺乏横断面T1序列的7例患者中,在矢状面T1序列上确认了脂肪平面的存在。
所有研究均使用1.5T磁体强度(magnet strength),但一例使用3.0T的磁体强度。
在椎间盘区域,测量脂肪的范围为:从棘突的的外层皮质到位于棘突中点处的椎旁肌的内缘(Fig.
4)。 








以前很少有研究专门比较不同的开放腰椎入路的结果。



在这种入路中,deep lumbar fascia在棘突的任一侧纵向切开,而不是直接在后正中线上切开,从而显示出paramidline的脂肪层。但是,我们注意到在他们的报告中没有很好地描述小关节(facets)的暴露。
多年来,我们一直在我们科使用同样的入路。Weatherley et
al.描述胸腰筋膜在棘上韧带的外侧被切开,并且椎旁肌通过Cobb elevator and a
gauze swab在骨膜下向外侧从棘突,椎板和小关节上剥离。 
为了便于后外侧融合,进一步对横突进行显露。




虽然我们发现对小关节的解剖出血较少,但在小关节外侧的解剖不太精确并且出血较多。
将这些肌腱与他们的附着点分离,并且识别中间的脂肪平面可以使这些外侧的小血管更容易可视化以进行电凝。
Weatherley et al.没有正式测量出血量。然而,我们认为这种方法是“最低限度的无出血入路”,有些出血是不可避免的,特别是在小关节的外侧进行解剖时。
虽然我们赞扬作者在减少出血方面的技巧,但我们不同意他们关于这种方法的一些陈述。我们不认为它是真正的无血管,由于在小关节外侧的血管解剖结构,一些出血是不可避免的。
Moghimi及其同事(原文作者)没有描述外侧的解剖。然而,根据我们的经验,这是解剖的一部分,并且是最容易出血的地方。
说明:
1. 参考自Grundy DJ.Skull traction and its complications.Injury,1983,15(3):173-7.
2. 参考自Surgery at the District Hospital: Obstetrics, Gynaecology, Orthopaedics and Traumatology(WHO; 1991; 207 pages)
3. 参考自亚历山大·范凯罗 (编者), 托德·阿尔伯特 (编者), 朱悦 (译者)《脊柱外科手术技巧》辽宁科学技术出版社.2010年
4. 参考自赵定麟《现代骨科手术学》上海世界图书出版公司.2012年

牵引的目的是使移位的颈椎恢复并保持正常序列状态,提供暂时的稳定并对脊髓间接减压。
这有益于促进神经功能恢复,避免加重神经损伤。
牵引通常是一个临时的措施,为进行更确实的治疗(手术固定)作准备。
颅骨牵引作为head-halter traction(对患者来说非常痛苦和不适)的替代方案,Crutchfield或Cone callipers(Fig. 10.3A) 的使用更容易且更舒适。
注:Crutchfield和Cone callipers是颅骨牵引的两种卡钳(callipers)。


head-halter traction的图示

Fig. 10.3. Skull traction. Cone callipers with spanner(扳手) (A); marking the scalp with two lines (B); sites for insertion of Crutchfield callipers (•) and Cone callipers (X) (C).
在进行颈椎骨折脱位牵引复位治疗前,医生必须注意可能存在不连续的多节段脊柱损伤。这就需要详细地了解病史和査体,也需要取得整个脊柱的完整的影像资料。
高质量的X线片或全脊柱CT是必要的。









无论牵引成功或失败,在手术切开复位或原位融合前需要进行MRI检査,以评价有无间盘突出或其他占位性病变,从而决定手术方式。
术前准备:
画线定位:

将callipers的中间正对头皮中线,将callipers放在横线上以标记进入点(Fig. 10.4A, B)。
或者矢状线与冠状线相交的中心点,沿冠状线向两侧4cm处各划一交线,即为牵引弓入口部位。
在头皮的横线上:


用1%利多卡因(1% lidocaine)浸润选定的部位后,沿着横线刺入直至颅骨(图10.4C,D)。


使用带有保护肩(drill bit with a protective
shoulder)的特殊钻头在颅骨外板上钻3-4mm深的孔,避免穿透颅骨内侧皮质(图10.4E-G)。钻头与颅骨的弧度成垂直方向钻穿颅骨外板。


- 当钻开外板时,会有一个落空感,然后接触到的就是内板。此时,就钻到位了,不能再往下钻了。
- 若钻头没有保护肩,可以自己做一个。用20ml针头套套在钻头上,钻头超过针头套约0.3~0.5cm。
- 必要时用CT测颅骨外板厚度。
- 手钻的使用方法。
插入卡尺的尖端并将其拧紧,使其牢固固定在颅骨上(图10.4H,I)。
用无菌纱布条覆盖伤口并施加适当的牵引力

图10.4
A,B.在插入Crutchfield callipers的位置做标记;
C.局麻药浸润头皮;
D,F,G.作一小切口,将钻头钻入颅骨;
E.钻头;
H-J.插入the points of the callipers并施加牵引




颅骨牵引的主要用途是矫正和维持颈椎因骨折而脱位的位置。对于未移位的骨折,它可以作为脊柱的夹板。






注意事项:
- 在小关节牵开前医生不应尝试手法复位,因为这往往会失败,并且有可能导致神经损害或关 节突骨折。
- 对于不稳定的牵张型损伤,不应使用直接轴向牵引。
- 如果神经功能恶化,则要停止手法复位,减少牵引重量。然后应安装Halo架,尽快进行MRI检査,以辨别是否有明显的脊髓受压。
halter traction在运送患者到医院的途中使用时,较为安全,但如果长期替代skull traction使用的话,可能会导致下颌处皮肤严重坏死。(Fig. 5)







说明:
1. 部分参考by Dr. Jacob Bickels MD, et al.Operative Techniques in Orthopaedic Surgical Oncology.LWW,2012.
患者仰卧位,消毒下肢及腹股沟区域(技术图1A)。
纵行长切口,沿缝匠肌起自大腿近端,远端直至胫骨结节(技术图1B)

A.右下肢巨大继发性软骨肉瘤。
应保持活检切口与下方肿瘤相连。原发肿瘤的常规入路是内侧切口,但必须切除外侧或前侧的切开活检通道并保持其与肿瘤的连续性。
找到并保护好隐神经(技术图1C)。

C.在切开皮肤及皮下组织后,筋膜下方后内侧为大块肌瓣。首先见到及需要保护的结构是隐神经。在大腿近端与股静脉伴行,沿缝匠肌至小腿。切断隐神经会导致小腿内侧麻木,有时会产生神经瘤引起痛疼。
沿缝匠肌及股内侧肌间隙进入,显露股动脉及与隐神经伴行的静脉(技术图1D,E)。


E.在大腿近端,向前外侧牵开缝匠肌可以显露股血管,如果需要可以显露至腹股沟韧带。
自近端向远端游离血管及隐神经,连同缝匠肌向后内侧牵开。
应用2-0或3-0丝线结扎全部供应股骨远端或肿瘤的血管(膝关节网)(技术图1F)。


F.应用2-0或3-0丝线结扎切断全部供应股骨远端或肿瘤的血管,可以减少失血,改善显露,确保血管的安全。
在Hunter管处应特别小心,因为血管位于收肌腱的深方。
在Hunter管远端游离腘血管并向后内侧牵开(技术图1G)。

G.在Hunter管,确认并切断收肌腱。主要血管就位于其下方,必须小心及耐心地分离血管。此处有一些侧副血管起自股血管,通向股骨及肿瘤,需要结扎切断。可见与缝匠肌伴行的隐神经。
可见股二头肌短头在大腿外侧由近端向远端与长头汇合。

显露并保护坐骨神经。
坐骨神经经梨状肌下孔出盆腔至臀大肌深面,在坐骨结节与大转子连线的中点深面下行入股后区,继而行于股二头肌长头的深面,达腘窝上角处分为胫神经和腓总神经两大终支。
在大腿肿瘤近端及内侧,切开收肌及股内侧肌结合部直至股骨,向外侧掀开股四头肌(技术图2A)。

A.在大腿近端肿瘤上方,收肌筋膜与股内侧肌筋膜汇合。切开这一间隙以显露股骨。股深血管位于收肌筋膜深方,沿股骨嵴(股骨粗线)方向走行。

在深方的内侧肌间隔处可见股深动脉及静脉终末端,可以结扎切断。
由肿瘤表面游离股血管、隐神经及腘血管至关节下方(技术图2B,C)。

B.在大腿近端,当向后内侧牵开缝匠肌后,可见隐神经伴行于股静脉。在切断收肌腱前,在膝关节下方显露并游离腘血管以确保其完整性。

C.完成内侧分离。隐神经由近端开始与缝匠肌伴行。股血管及腘血管已经分离,在大腿的远端与缝匠肌和隐神经伴行。
切断腓肠肌内侧头,必须保护好内侧腓肠血管(技术图2D,E)。

D.在膝关节内侧,分离并切断腓肠肌内侧头。

E.显露并切断内侧膝关节血管。

当完全游离并牵开股血管后,连同髌骨、髌腱向外侧掀开全部或部分股四头肌,此时股中间肌可以作为非常理想的肿瘤学边界。
通常行关节内切除。
应用电刀切开关节囊,切断前后交叉韧带、腘肌腱及侧副韧带。 

在可以直视腘血管或术者应用手指保护好腘血管后,切开后关节囊。
肿瘤很少侵犯关节;如果出现,肿瘤会被滑膜所覆盖。
如果出现局部复发,常出现在神经血管束游离平面,而并不是在膝关节水平。
由肿瘤表面掀开股四头肌,在肿瘤上方保留一层肌肉作为肿瘤学边界。将股中间肌保留在肿瘤表面作为肿瘤学边界(技术图2F)。

F.切开关节,由肿瘤表面掀开股四头肌,将股中间肌保留在肿瘤表面作为肿瘤学边界。
做如下皮质标记:

G.在确定截骨平面的近端及远端的股骨和胫骨上进行皮质标记,在肿瘤切除前及假体重建后分别测量长度。此时在前方皮质做标记帮助旋转对线。
应用电锯在术前计划的水平截断股骨(技术图3A-C)。应比假体的股骨部分长度多截除1cm股骨,随后只需截除7mm厚的胫骨。这1.7cm的差距,是假体组装时假体股骨髁与下方的全聚乙烯胫骨部分之间的距离,这样才能保证下肢等长(技术图4A)。

A.应用线锯或摆锯在术前计划的平面,股骨皮质标记下方截断股骨。B.C.截除股骨标本与假体前后位大体像。

或者可以应用厂商提供的模具直接截除17mm的胫骨,这样就可以根据股骨假体的实际长度截除股骨。这样可以使髌骨位于更加接近自然解剖位置,对于术后功能没有影响(技术图4B)。

B.胫骨近端只需要截除7mm。这可以为假体胫骨部分提供最大的平台。一期重建常规应用8mm全聚乙烯胫骨假体。由金属股骨髁至8mm全聚乙烯胫骨假体下缘的间距是1.7cm。这可以保证下肢长度差别在1cm之内。不需要确保髌骨在膝关节的位置。髌骨的活动轨迹及功能非常重要,但通常术后都恢复的非常良好。
对近端股骨髓腔行术中冰冻活检。
髓腔锉扩髓直至股骨髓腔可以接受假体柄最大径。
随后应用凸面挫(acing reamer)挫凹截骨面,冲洗刷(irrigating brush)冲洗(技术图4C-E)。

C.术中冰冻报告提示切缘阴性后,应用持骨器把持股骨,髓腔锉扩髓。应用锋利的髓腔锉缓慢轻柔地扩髓,同时大量冲洗以避免脂肪栓塞。扩大髓腔直至假体柄的最大部分可以轻松地插入。
D.应用凸面挫准备截骨面。

E.应用冲洗刷缓慢轻柔地再次清理髓腔。
如果应用骨水泥固定,此时可以安放近端骨水泥限制器(A proximal cement restrictor)。

应用摆锯稍稍向后上方倾斜(slight posterior slope)(后方高)截除胫骨(技术图4F,G)。这一操作可以徒手完成,现在也可以应用器械辅助完成。

F.徒手应用摆锯截除7mm胫骨近端。厂商目前可以提供胫骨截骨模具,可以截除较大块的胫骨,以确保髌骨位于关节线处。

G.通常应在矫正器远端指向第2跖骨时,垂直截除胫骨。截除胫骨时应使后方稍高,以保证假体充分的伸直。如果前方高,会对患者造成膝关节屈曲挛缩。

准备好胫骨近端以安装假体胫骨部分。
此时可以安装胫骨远端骨塞或骨水泥限制器(distal bone plug or cement restrictor)。
插入全聚乙烯胫骨假体试模(A trial all-poly tibial prosthesis)。
术中拍片以确保截骨面与胫骨干垂直,没有内翻或外翻。
安装假体试模本身也是避免内外翻的方法(技术图4H)。

H.行术中平片确保截骨面垂直。很小的内翻或外翻并不影响术后功能或导致松动。
切除约50%的关节下脂肪垫以防止术后冲击。这可能会造成术后的即时疼痛。
切除髌骨关节面,应用磨钻磨除以安装假体髌骨部分。


I.应用摆锯切除髌骨面。
J.应用磨钻钻孔,准备安装单中心钉全聚乙烯髌骨假体。
K.目前可以应用模具准备胫骨。可以见到备好的胫骨及髌骨。
L.髌骨试模超出了髌骨范围,应该应用更小的试模替换。
试安装假体并测量,以确保重建后的长度与切除前长度一致(技术图4M)。

M.测量股骨及胫骨标志间的重建后长度,确保其与切除前长度相等。此时应检查踝部脉搏。
检查关节活动度:股四头肌及髌骨的活动轨迹应非常满意,没有外侧脱位的倾向。
此时如果有髌骨半脱位或脱位的倾向,应做适当的外侧松解。
同时应检查股血管的张力
需要避免假体过长
应用单中心钉聚乙烯假体,修饰截骨面以适合固定。
髌骨表面置换可以允许即刻的有一定强度的康复锻炼,并不需要考虑由于髌骨软骨与金属远端假体研磨所造成的膝关节疼痛。

如果预期膝关节主动活动度达到屈曲120°〜130°,完全伸直且没有伸肌滞后(full
extension, and no extensor
lag),髌骨表面置换则非常重要,并且通常可以达到这些要求。 
如果预期膝关节主动活动度≤90°,是否行髌骨表面置换则没有太大的区别。


缝合前应非常仔细地止血。
充分应用抗菌溶液冲洗伤口,最后一次应用生理盐水冲洗。
将关节囊尽量缝合于胫骨近端残留的关节囊组织。
安置深部10mm引流管后,应用#1可吸收线将缝匠肌与股内侧肌缝合(技术图6)。

闭合伤口:安放2根10mm引流管自近端引出。将缝匠肌与残余的股内侧肌缝合。远端缝合关节囊。
安置浅层10mm引流管后,缝合皮下组织。
缝线固定引流管,至24h引流量小于30〜40ml
可以应用钉皮器或皮下缝合闭合皮肤。
在不到1%的病例中会应用到腓肠肌瓣,但是当没有足够的软组织时,这种肌瓣非常有帮助覆盖假体。
无菌敷料覆盖伤口绷带包扎(Ace wrap)。

患者在床上应用持续被动活动装置(continuous passive motion machine,CPM)

患足穿持续性压力鞋(Sequential compression boots)。 
说明:
1. 翻译自Sultan S, Morawa E, Niesvizky R,et al. Necrotizing Soft Tissue Infection in Two Patients with Multiple Myeloma.Surg Infect (Larchmt),2011,12(5):391-5.
坏死性软组织感染(Necrotizing soft tissue infection,NSTI)的发病率和死亡率都非常高,特别是在免疫功能低下的患者(immunocompromised patients)中
例如多发性骨髓瘤患者
早期诊断和治疗至关重要,但在症状不典型和机体防御功能受损的患者中,诊断和治疗尤为复杂和困难。
药物治疗:
出于对NSTI的担心,对其踝关节进行了下述手术以治疗关节积脓(Fig. 1A):
紧急清创术(debridement)
筋膜切除术(fasciectomy)
关节切开术/冲洗术(arthrotomy/washout of the ankle joint)

他在手术后被送到外科重症监护室(SICU),在那里他开始使用drotrecogin alfa (activated)。
Drotrecogin alfa是human activated protein C的重组形式,具有抗血栓形成,抗炎和促纤维蛋白溶解的特点。尚未发现Drotrecogin alfa可改善严重脓毒症患者的预后。
一天后,他再次进入手术室进行进一步较小范围的清创(minimal further debridement)。此时,感染源已经被控制。
从初次手术期间采集的血液培养物和初次手术中采集的组织培养物中获得的培养结果为化脓性链球菌(Streptococcus pyogenes),因此抗生素改为克林霉素(clindamycin)和青霉素G(penicillin G)。
放置VAC(vacuum-assisted closure,VAC)敷料以促进伤口愈合。 



肿胀(swelling)(75%)
超出红斑边缘的疼痛(pain beyond the margins of erythema)(73%)
红斑(erythema)(66%)
然而,这些发现是敏感的,但不是NSTI特有的。

病例1只有一个平片:显示“软组织肿胀”
病例2进行了非增强的CT平扫:显示皮下组织弥漫性水肿,报告为“可能的蜂窝织炎”,但没有气体或局部的聚集。

Images show a pedunculated area of skin thickening with a radial pattern of edema in the subcutaneous fat of the medial left thigh.
上述两例患者都没有任何典型的影像学特征:
X线显示的皮下气肿(subcutaneous emphysema) 
CT显示的筋膜增厚(fascial thickening) 
据我们所知,NSTI的文献中只有两篇关于其使MM复杂化。